Circadian health
Circadian rhythm, aging, and dementia
As we age, the internal clock that runs sleep, alertness, and repair grows quieter and harder to set, and the eye itself lets in less of the blue light that keeps that clock on time. In people living with dementia, the breakdown shows up as broken sleep, daytime drowsiness, and the evening agitation called sundowning. Giving older eyes enough of the right light, at the right hour, can help steady these rhythms. The hard part is that a parlor that looks perfectly well lit to a visitor can be reaching an 80-year-old’s clock at a fraction of the dose, and nothing in the room betrays it.
The connection
The body’s master clock (the suprachiasmatic nucleus, SCN) is set each day mainly by light reaching specialized retinal cells (ipRGCs). Two things go wrong at once with age: the SCN loses signaling neurons and its output rhythm flattens, while the lens yellows and the pupil narrows, so far less short-wavelength light reaches those clock-setting cells. Older adults in care settings also tend to get very little bright daytime light to begin with.
The upshot is a weaker rhythm, shifted earlier and poorly held in place. In Alzheimer’s disease and related dementias the same changes run deeper, and circadian disruption looks like not only a result of the disease but possibly an early contributor to it (Leng et al., 2019).
The science
Healthy older adults show an advanced circadian phase (earlier bed and wake times), a flatter rhythm, and more fragmentation. Post-mortem work finds a selective loss of SCN neurons expressing arginine vasopressin and vasoactive intestinal peptide, matching the dysfunction (Leng et al., 2019).
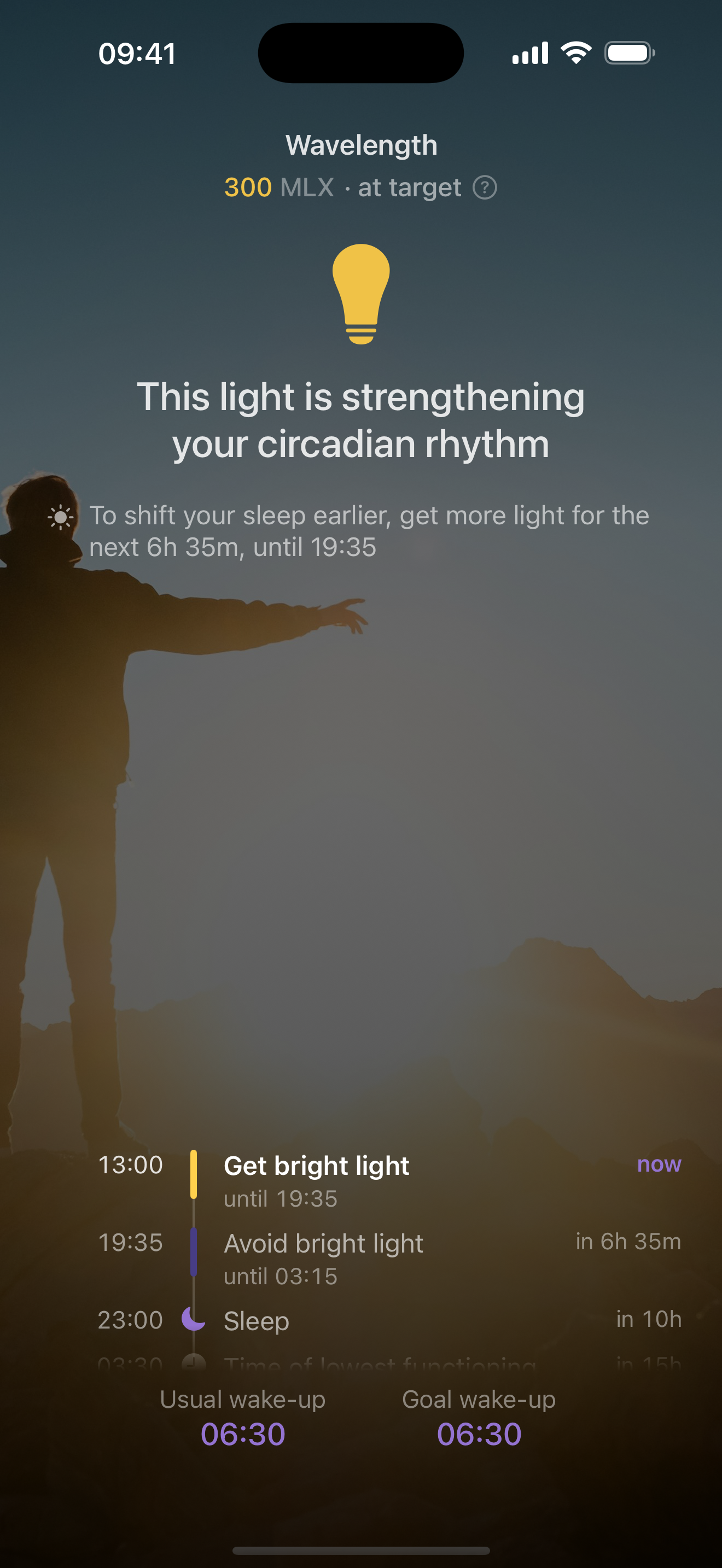
The eye is the second bottleneck. The lens yellows over the years, screening out exactly the violet and blue wavelengths that drive the clock-setting pathway. Turner and Mainster (2008) estimate a 10-year-old has roughly ten times the circadian photoreception of a 95-year-old, already down to about half by age 45. Add a smaller pupil, and an older person in a normally lit room may not be getting a signal strong enough to anchor the clock. This is the core reason older eyes need more light, not less, and the reason a parlor a visitor reads as well lit has to be checked with a meter rather than a glance; a phone app like Wavelength reads the melanopic lux landing at the eye from an iPhone.
The dementia link runs both ways. Sleep drives the brain’s clearance of metabolic waste; in mice, amyloid-beta clears roughly twice as fast during sleep (Xie et al., 2013). Run the clock the other way and plaque deposition speeds up in models, while in people, rest-activity fragmentation shows up in the preclinical phase of Alzheimer’s (Leng et al., 2019). Sundowning, seen in an estimated 20 to 45 percent of people with Alzheimer’s, is widely thought to reflect this SCN and melatonin disruption.
What the research shows
The landmark trial is Riemersma-van der Lek et al. (2008), a double-blind RCT of 189 residents (mean age 85.8, 87 percent with dementia) run over about 15 months. Whole-day bright light (about 1000 lux) slowed cognitive decline by 0.9 MMSE points and cut depressive symptoms by about 19 percent. Melatonin alone shortened sleep-onset latency but worsened mood on its own; the authors concluded melatonin should only be paired with light.
Tailored lighting, engineered to put a defined dose at the eye, did more consistently well. Figueiro et al. (2014) delivered roughly 300 to 400 lux at the eye and improved Pittsburgh Sleep Quality Index scores from 8.7 to 4.1, depression from 12.0 to 6.0, and agitation. The larger randomized crossover RCT (Figueiro et al., 2019; 46 participants) cut PSQI scores from 10.30 to 6.67 and eased depression and agitation against control.
The evidence is real, but do not oversell it. A systematic review found benefits sitting alongside uneven methods and mixed results (Goudriaan et al., 2021). The honest version: enough daytime light is a low-risk, evidence-backed way to support sleep, mood, and a steadier rhythm, but it is a supportive measure, not a cure, and the effect varies by person and setting.
Frequently asked questions
Why do older adults need more light than younger people to stay on a healthy sleep schedule?
The lens yellows with age and the pupil narrows, so far less of the blue light that sets the clock reaches the retina. By the 80s, circadian photoreception can be roughly a tenth of a child’s, so older eyes need more daytime light to land the same clock signal.
Can bright light help with dementia symptoms like agitation and poor sleep?
Several trials show daytime bright or circadian-tuned light can improve sleep, mood, and agitation in people with dementia. Results vary by study and by person, and light is a supportive measure, not a cure.
What is sundowning and is it related to the body clock?
Sundowning is rising confusion and agitation in the late afternoon and evening, affecting an estimated 20 to 45 percent of people with Alzheimer’s. It is widely linked to disruption of the SCN master clock and the melatonin system, which is why steadying rhythms with light is studied as a possible aid.
Does poor sleep contribute to Alzheimer’s, or is it just a symptom?
It appears to run both ways. Sleep helps clear amyloid-beta from the brain, and circadian disruption can both follow from and possibly precede neurodegeneration, with rest-activity fragmentation showing up in the preclinical phase of Alzheimer’s.
How much daytime light should an older adult get, and how do I know if they are getting enough?
Aim for at least the 250 melanopic lux daytime target at the eye, and treat it as a floor given age-related lens changes. Indoor light is often far dimmer than it looks, so a melanopic-lux reading taken at the eye is the only reliable way to confirm the dose is actually landing.
References
- Brown TM, et al. (2022). Recommendations for daytime, evening, and nighttime indoor light exposure. PLOS Biology.
- Leng Y, et al. (2019). Association between circadian rhythms and neurodegenerative diseases. The Lancet Neurology.
- Riemersma-van der Lek RF, et al. (2008). Effect of bright light and melatonin on cognitive and noncognitive function in elderly residents of group care facilities: a randomized controlled trial. JAMA.
- Figueiro MG, et al. (2014). Tailored lighting intervention improves measures of sleep, depression, and agitation in persons with Alzheimer’s disease. Clinical Interventions in Aging.
- Figueiro MG, et al. (2019). Effects of a tailored lighting intervention on sleep quality, rest-activity, mood, and behavior in older adults with Alzheimer disease: a randomized clinical trial. Journal of Clinical Sleep Medicine.
- Turner PL, Mainster MA (2008). Circadian photoreception: ageing and the eye’s important role in systemic health. British Journal of Ophthalmology.
- Xie L, et al. (2013). Sleep drives metabolite clearance from the adult brain. Science.
- Goudriaan I, et al. (2021). Dementia enlightened?! A systematic review of indoor environmental light and the health of older persons with dementia in long-term care. Clinical Interventions in Aging.
Related guides
Wavelength is a wellness and education tool, not a medical device. This page summarizes published research and is not medical advice. Consult a qualified clinician about any health condition or before starting light therapy.